


Lloyd’s Corner: Ectopic until proven otherwise
Here is a case from Dr Lloyd Gordon from Humber in Toronto:
A women in her late 30s presented with a sudden onset of lower abdominal pain that started couple of hours before. She had some sort of ovarian surgery years ago. The LNMP was a week or two ago and she didn’t think she was pregnant. Hmmm…
The Head Nurse asked me to see the patient next as she was concerned about her. She seemed to be in pain but was calm, maybe a bit pale. Pulse 103. BP OK. Tender but not peritoneal.
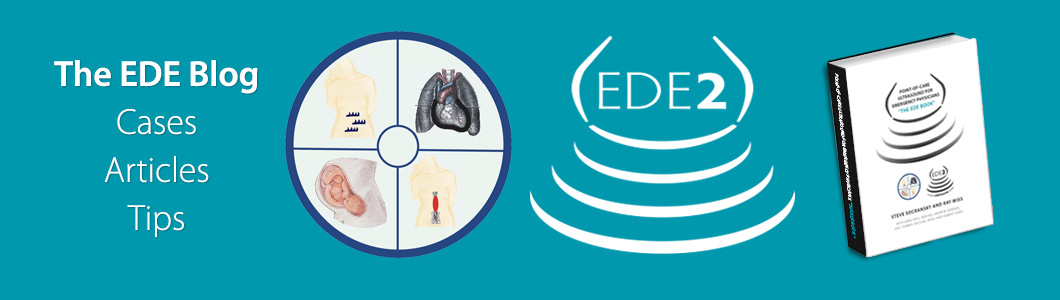
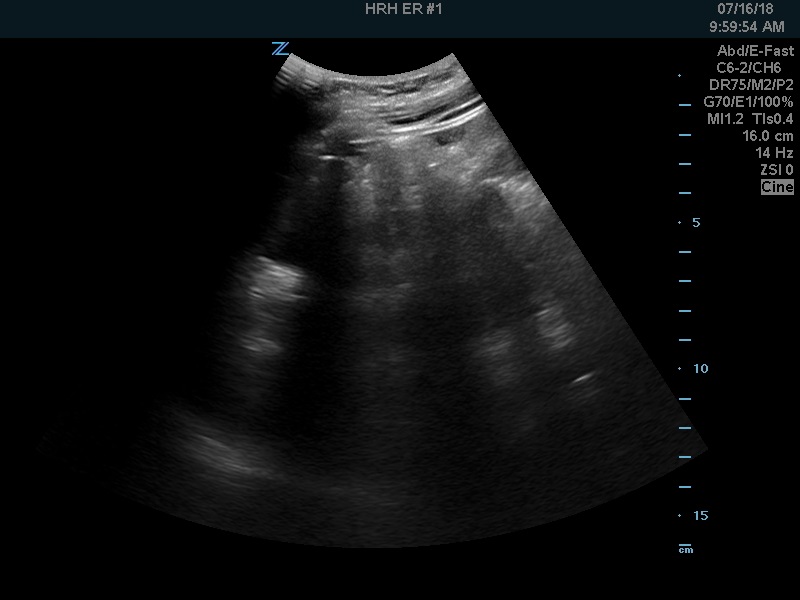
After examining her I started by scanning for free fluid. Here is the RUQ:
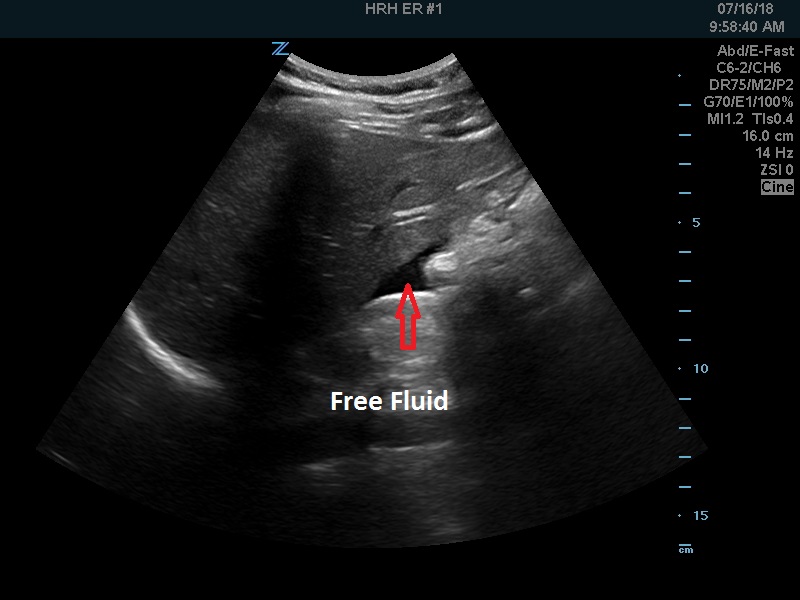
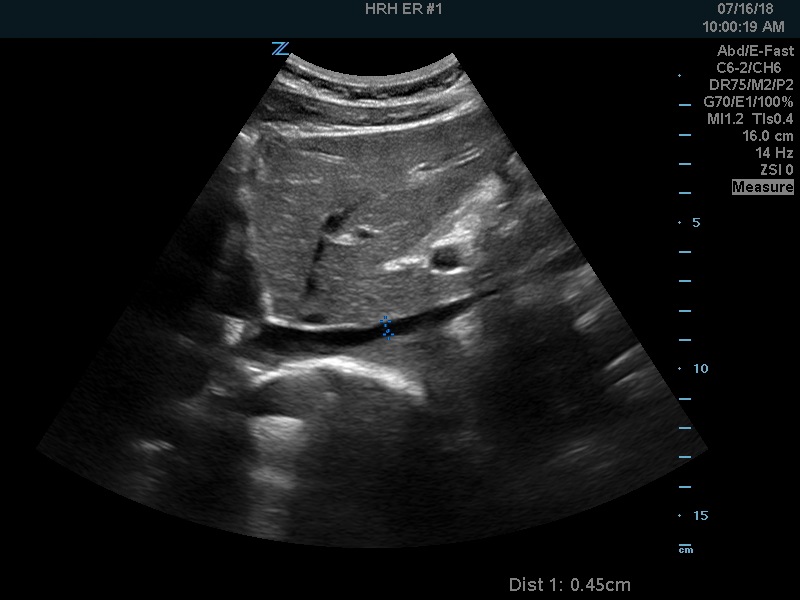
And the LUQ:
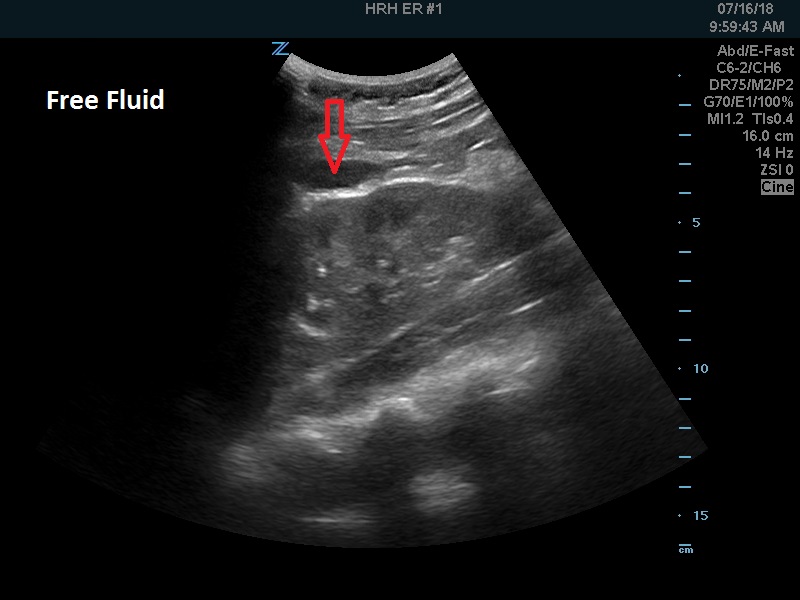
Not that much, but positive. Onto the pelvis…
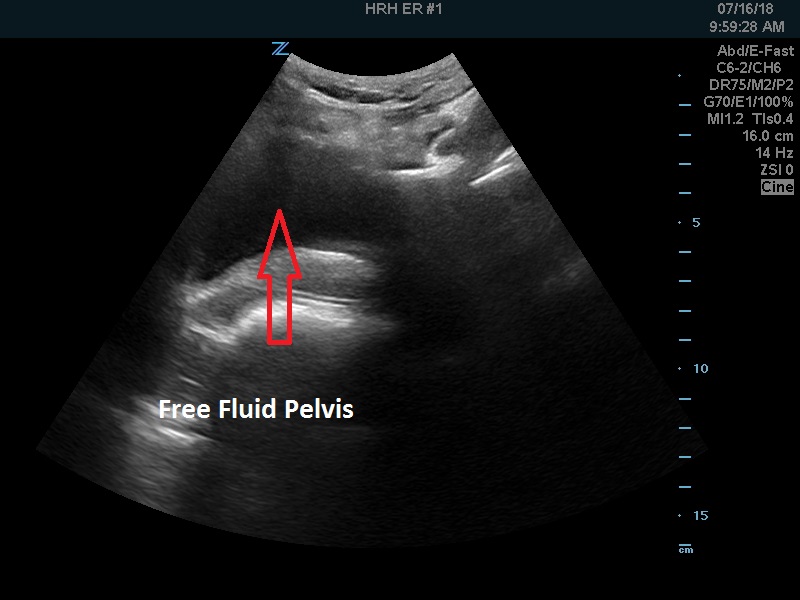
Free fluid more pronounced in the pelvis. The uterus was empty (not shown).
Pelvic views showed what I call a “Sturm and drang” appearance or colloquially a “mess”, blood clots and tissue…
The IVC was very narrow for a young, healthy woman.
She didn’t look too bad at that point so I ordered a 2 liter NS bolus and called Gyn and asked him to take her right to the OR.
A few minutes later the Nurses said she was having a seizure. At this point she was absolutely white. I ordered 2 units of uncrossmatched O- blood under pressure. Within a few minutes the O&G came. The B-HCG was negative but the treatment was the same: immediate laparoscopy! At surgery they removed a haemorrhagic ovarian cyst and a lot of blood from the pelvis and paracolic gutters.
So not an ectopic but in a young woman, a positive FAST and shock needs the same immediate treatment. The + EDE/POCUS gave me the confidence to ask the Gyn to take her right to the OR.
Editor’s note: There are barriers to doing POCUS on shift. One set of barriers falls into the cognitive category. What would have dissuaded us from not picking up the probe in a case like this? Patient in late 30s. Patient says she is not pregnant so why would POCUS be useful? Not hypotensive. Lots of lower abdo pain cases in this demographic…wasting time to scan all of them? Clues that you should pick up the probe: charge RN worried about patient. Significant pain. Tachycardia. Patient still has uterus. Maybe has ovarian abnormalities given prior ovarian surgery.